
As the Department of Defense continues its massive reorganization of the military health system, a government watchdog says the Defense Health Agency needs to reevaluate its staffing systems and administrative plans, citing concerns that they will result in too few health care providers and too many administrators.
In a report released Aug. 21, the Government Accountability Office recapped the multiyear effort to reorganize the military health system under the Defense Health Agency, an effort which Congress kicked off in 2016 in an effort to create a more efficient oversight structure for military treatment facilities (MTF, the term for military hospitals, medical centers, and clinics), lower costs, and improve care.
GAO described the project as one of the largest reorganizations in the history of the Department of Defense, and one which the Surgeons General of the Army and Air Force called “extremely difficult,” and “a complicated merger of four cultures.” The result of the change is that DHA oversees day-to-day health care delivery at each MTF, which is staffed by a mix of civilian and military medical providers, while the military departments are responsible for assigning military providers to MTFs.
The ambitious transition of authorities was completed in 2022, but GAO found persistent challenges regarding medical staff levels and DHA’s estimates for administrative personnel.
Medical Staff Shortfalls
GAO reported that medical staff shortfalls have been a problem in both the military and civilian sectors for years. In the military, the shortfalls are exacerbated by the fact that uniformed providers often must travel for training, deployments, or rotations to other duty assignments. Officials at Naval Hospital Jacksonville, Fla., told GAO that military provider shortfalls jeopardized their ability to provide 24/7 emergency room services in the summers of 2022 and 2023.
Contributing to the shortfalls could be the fact that the military departments retain authority and responsibility for assigning military providers to MTFs and deploying them elsewhere. The long hiring and contracting processes for civilians also leaves vacancies unfilled.
DHA is attempting to mitigate the problem by moving civilian providers between facilities to fill vacancies; by allowing military departments to support each other with providers; by establishing a new oversight mechanism to analyze shortages; and creating a new human capital distribution framework. However, GAO urged DHA to develop a strategic total workforce plan to better tailor and monitor its long-term plans towards reducing provider gaps and mitigate the effect of deployments on MTF operations.
While the DOD agreed with GAO’s recommendations, it has yet to implement them, saying that the ongoing military health system reforms are still in flux. GAO pushed back, arguing that until the recommendations are implemented, “DHA may continue to face shortfalls in personnel that challenge MTF operations.”
More Administrators Than Necessary?
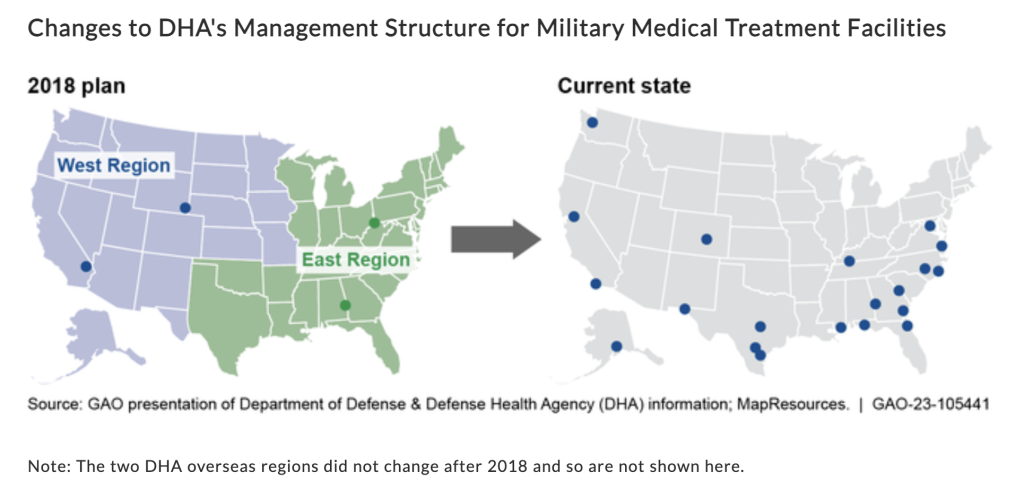
When DHA began managing and administering military treatment facilities, it also grouped more than 700 worldwide MTFs into two U.S. regions with two offices each as part of a 2018 plan. That plan was replaced in 2019, however, with a new arrangement of 36 markets in the U.S., two regions overseas, and 22 offices to manage them.
GAO argued the Department of Defense needs to reevaluate its new plan, especially considering the DHA’s estimate for 1,400 personnel to staff its 22 offices is “higher than what is needed to support the offices’ workload, and the number exceeds expected budgetary and personnel resources,” the GAO wrote.
The Department of Defense has struggled to understand its DHA headquarters personnel requirement for years, GAO noted, but the department has yet to conduct a comprehensive review to nail down the right number. Staffing shortfalls also affect the offices, with a “coalition of the willing” from the MTFs stepping up to support office tasks, GAO wrote. Until such an evaluation takes place, DHA “may risk not accomplishing its vision for an integrated health system that efficiently uses resources and lowers costs,” GAO wrote.
More Changes
Besides the ongoing changes under DHA, the Air Force Medical Service (AFMS) on Aug. 11 announced its own sweeping reorganization. The service will establish two regional Air Force Medical Commands called AFMED Regions. The new structure will allow two medical Air Force general officers to elevate any concerns from the wing and medical group commander level to the Air Force Surgeon General or DHA leadership. The layout will encourage “streamlined strategic and operational engagement to maximize health support,” Col. Patrick Parsons, Military Health System Governance Liaison Officer for AFMS, said in a press release.
The Air Force hopes the regional commands, overseen by the Air Force Surgeon General, will better align service command and control authorities with DHA; enable senior Air Force medical leaders to better advocate for Air Force and Space Force MTFs; and better support Air Force and Space Force medical readiness priorities.
“The aim with AFMED is to provide clear direction to local leaders at the installation on health care and readiness priorities to ensure they spend less time deconflicting policies and can focus on the mission and their people,” Stephen Mounts, Air Force Associate Deputy Surgeon General, said in the press release.
Officials said Air Force medical providers should not see an impact in their day-to-day work. The goal is to establish the two AFMEDs with initial operating capability by October 1. The Air Force Surgeon General’s Office could not immediately answer a question from Air & Space Forces Magazine about whether GAO’s concerns about DHA staffing and efficiency played a role in the AFMED plan, but it appears the Department of the Air Force is working to keep pace with the changes in military health over the past several years.
“Having navigated the challenges of the MHS transition since 2017, our Air Force leadership asked us to improve our ability to execute the mission, and AFMED is the answer,” Lt. Gen. Robert Miller, Air Force Surgeon General, said in the release.